Pharmacotherapeutic group: Calcium channel blockers, selective calcium channel blockers with mainly vascular effects, dihydropyridine derivates.
ATC code: C08CA01.
Pharmacology: Pharmacodynamics: Amlodipine is a calcium ion influx inhibitor of the dihydropyridine group (slow channel blocker or calcium ion antagonist) and inhibits the transmembrane influx of calcium ions into cardiac and vascular smooth muscle.
The mechanism of the antihypertensive action of amlodipine is due to a direct relaxant effect on vascular smooth muscle. The precise mechanism by which amlodipine relieves angina has not been fully determined but amlodipine reduces total ischaemic burden by the following two actions: Amlodipine dilates peripheral arterioles and thus, reduces the total peripheral resistance (afterload) against which the heart works. Since the heart rate remains stable, this unloading of the heart reduces myocardial energy consumption and oxygen requirements.
The mechanism of action of amlodipine also probably involves dilatation of the main coronary arteries and coronary arterioles, both in normal and ischaemic regions. This dilatation increases myocardial oxygen delivery in patients with coronary artery spasm (Prinzmetal's or variant angina).
In patients with hypertension, once daily dosing provides clinically significant reductions of blood pressure in both the supine and standing positions throughout the 24 hour interval. Due to the slow onset of action, acute hypotension is not a feature of amlodipine administration.
In patients with angina, once daily administration of amlodipine increases total exercise time, time to angina onset, and time to 1 mm ST segment depression, and decreases both angina attack frequency and glyceryl trinitrate tablet consumption.
Amlodipine has not been associated with any adverse metabolic effects or changes in plasma lipids and is suitable for use in patients with asthma, diabetes, and gout.
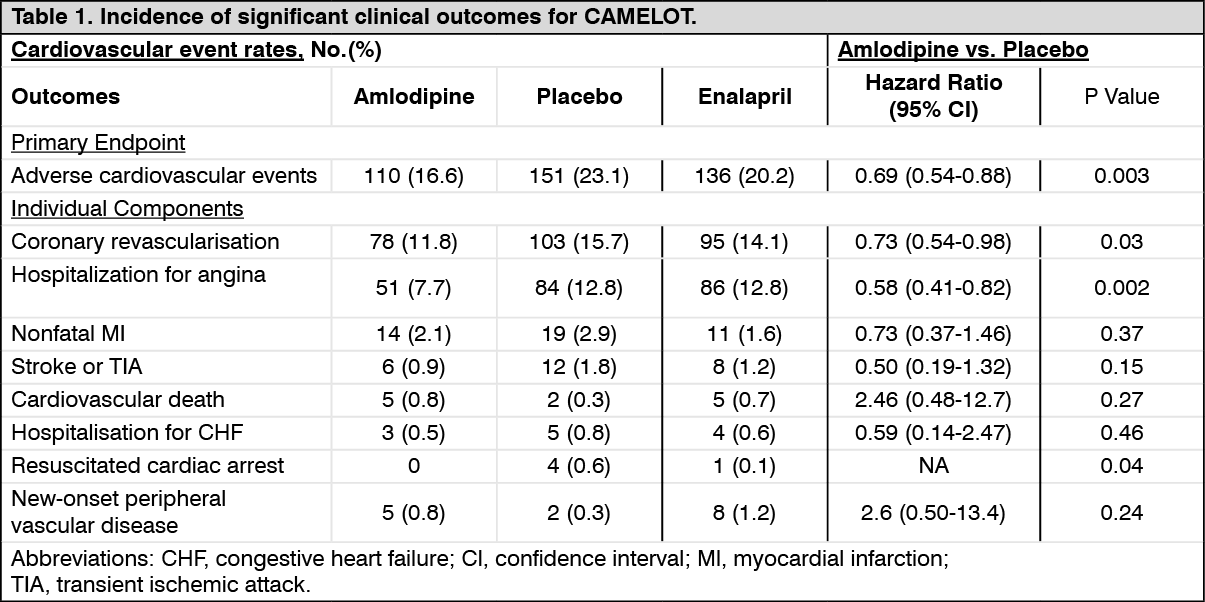
Use in patients with coronary artery disease (CAD): The effectiveness of amlodipine in preventing clinical events in patients with coronary artery disease (CAD) has been evaluated in an independent, multicentre, randomised, double-blind, placebo-controlled study of 1997 patients; Comparison of Amlodipine vs. Enalapril to Limit Occurrences of Thrombosis (CAMELOT). Of these patients, 663 were treated with amlodipine 5-10 mg, 673 patients were treated with enalapril 10-20 mg, and 655 patients were treated with placebo, in addition to standard care of statins, beta-blockers, diuretics and aspirin, for 2 years. The key efficacy results are presented in Table 1. The results indicate that amlodipine treatment was associated with fewer hospitalisations for angina and revascularisation procedures in patients with CAD. (See Table 1.)
 Click on icon to see table/diagram/image
Use in patients with heart failure:
Click on icon to see table/diagram/image
Use in patients with heart failure: Haemodynamic studies and exercise based controlled clinical trials in NYHA Class II-IV heart failure patients have shown that amlodipine did not lead to clinical deterioration as measured by exercise tolerance, left ventricular ejection fraction and clinical symptomatology.
A placebo controlled study (PRAISE) designed to evaluate patients in NYHA Class III-IV heart failure receiving digoxin, diuretics and ACE inhibitors has shown that amlodipine did not lead to an increase in risk of mortality or combined mortality and morbidity with heart failure.
In a follow-up, long-term, placebo-controlled study (PRAISE-2) of amlodipine in patients with NYHA III and IV heart failure without clinical symptoms or objective findings suggestive or underlying ischaemic disease, on stable doses of ACE inhibitors, digitalis, and diuretics, amlodipine had no effect on total cardiovascular mortality. In this same population amlodipine was associated with increased reports of pulmonary oedema.
Treatment to prevent heart attack trial (ALLHAT): A randomised double-blind morbidity-mortality study called the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) was performed to compare newer drug therapies: amlodipine 2.5-10 mg/d (calcium channel blocker) or lisinopril 10-40 mg/d (ACE-inhibitor) as first-line therapies to that of the thiazide-diuretic, chlorthalidone 12.5-25 mg/d in mild to moderate hypertension.
A total of 33,357 hypertensive patients aged 55 or older were randomised and followed for a mean of 4.9 years. The patients had at least one additional CHD risk factor, including: previous myocardial infarction or stroke (>6 months prior to enrolment) or documentation of other atherosclerotic CVD (overall 51.5%), type 2 diabetes (36.1%), HDL-C <35 mg/dl (11.6%), left ventricular hypertrophy diagnosed by electrocardiogram or echocardiography (20.9%), current cigarette smoking (21.9%).
The primary endpoint was a composite of fatal CHD or non-fatal myocardial infarction. There was no significant difference in the primary endpoint between amlodipine-based therapy and chlorthalidone-based therapy: RR 0.98 95% CI (0.90-1.07) p=0.65. Among secondary endpoints, the incidence of heart failure (component of a composite combined cardiovascular endpoint) was significantly higher in the amlodipine group as compared to the chlorthalidone group (10.2% vs. 7.7%, RR 1.38, 95% CI [1.25-1.52] p<0.001). However, there was no significant difference in all-cause mortality between amlodipine-based therapy and chlorthalidone-based therapy. RR 0.96 95% CI [0.89-1.02] p=0.20.
Use in children (aged 6 years and older): In a study involving 268 children aged 6-17 years with predominantly secondary hypertension, comparison of a 2.5 mg dose, and 5 mg dose of amlodipine with placebo, showed that both doses reduced Systolic Blood Pressure significantly more than placebo. The difference between the two doses was not statistically significant.
The long-term effects of amlodipine on growth, puberty and general development have not been studied. The long-term efficacy of amlodipine on therapy in childhood to reduce cardiovascular morbidity and mortality in adulthood have also not been established.
Pharmacokinetics: Absorption, distribution, plasma protein binding: After oral administration of therapeutic doses, amlodipine is well absorbed with peak blood levels between 6-12 hours post dose. Absolute bioavailability has been estimated to be between 64 and 80%. The volume of distribution is approximately 21 L/kg.
In vitro studies have shown that approximately 97.5% of circulating amlodipine is bound to plasma proteins.
The bioavailability of amlodipine is not affected by food intake.
Biotransformation/elimination: The terminal plasma elimination half life is about 35-50 hours and is consistent with once daily dosing.
Amlodipine is extensively metabolised by the liver to inactive metabolites with 10% of the parent compound and 60% of metabolites excreted in the urine.
Use in hepatic impairment: Very limited clinical data are available regarding amlodipine administration in patients with hepatic impairment. Patients with hepatic insufficiency have decreased clearance of amlodipine resulting in a longer half-life and an increase in AUC of approximately 40-60%.
Use in older patients: The time to reach peak plasma concentrations of amlodipine is similar in older and younger subjects.
Amlodipine clearance tends to be decreased with resulting increases in AUC and elimination half-life in older patients. Increases in AUC and elimination half-life in patients with congestive heart failure were as expected for the patient age group studied.
Use in children: A population PK study has been conducted in 74 hypertensive children aged from 1 to 17 years (with 34 patients aged 6 to 12 years and 28 patients aged 13 to 17 years) receiving amlodipine between 1.25 and 20 mg given either once or twice daily. In children 6 to 12 years and in adolescents 13-17 years of age the typical oral clearance (CL/F) was 22.5 and 27.4 L/hr respectively in males and 16.4 and 21.3 L/hr respectively in females. Large variability in exposure between individuals was observed. Data reported in children below 6 years is limited.
Toxicology: Preclinical safety data: Reproductive toxicology: Reproductive studies in rats and mice have shown delayed date of delivery, prolonged duration of labour and decreased pup survival at doses approximately 50 times greater than the maximum recommended dose for humans based on mg/kg.
Impairment of fertility: There was no effect on the fertility of rats treated with amlodipine (males for 64 days and females 14 days prior to mating) at doses up to 10 mg/kg/day (8 times* the maximum recommended human dose of 10 mg on a mg/m
2 basis). In another rat study in which male rats were treated with amlodipine besilate for 30 days at a dose comparable with the human dose based on mg/kg, decreased plasma follicle-stimulating hormone and testosterone were found as well as decreases in sperm density and in the number of mature spermatids and Sertoli cells.
Carcinogenesis, mutagenesis: Rats and mice treated with amlodipine in the diet for two years, at concentrations calculated to provide daily dose levels of 0.5, 1.25, and 2.5 mg/kg/day showed no evidence of carcinogenicity. The highest dose (for mice, similar to, and for rats twice* the maximum recommended clinical dose of 10 mg on a mg/m
2 basis) was close to the maximum tolerated dose for mice but not for rats.
Mutagenicity studies revealed no drug related effects at either the gene or chromosome levels.
*Based on patient weight of 50 kg.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out